






Living with Food Allergies

Food Allergy Facts and Figures
Understanding food allergy is crucial for effective advocacy and support. By raising awareness and promoting education, we can empower communities to act and improve food allergy rates, treatments, and care.
Kids with Food Allergies (KFA) promotes healthy and inclusive living for families managing food allergies. KFA is part of the nation’s oldest and largest asthma and allergy charity, the Asthma and Allergy Foundation of America (AAFA).
What Is a Food Allergy?
What Are the Symptoms of Food Allergies?
How Common Are Food Allergies?
What Are the Most Frequent Food Allergens?
How Are Food Allergies Managed and Treated?
How Many People Seek Medical Care for Anaphylaxis?
Do People Die from Anaphylaxis or Food Allergy?
What Are the Economic Costs of Food Allergy?
Are Food Allergies Outgrown?
What Is a Food Allergy?
- A food allergy occurs when the body’s immune system sees a certain food as harmful and reacts by causing specific clinical symptoms. This is an allergic reaction.
- Foods that cause allergic reactions are called allergens. People are usually allergic to proteins found in a food allergen.
- There are 2 types of food allergies:
- Immunoglobulin-E-mediated (IgE-mediated): With this type of food allergy, the body’s immune system makes antibodies called immunoglobulin E (IgE). IgE antibodies react with a certain food and cause immediate symptoms.
Examples include:- Peanut allergy
- Milk allergy
- Egg allergy
- Shellfish allergy
- Fish allergy
- Tree nut allergy
- Wheat allergy
- Soy allergy
- Sesame allergy
- Cell-mediated: Immune cells that do not involve IgE antibodies react to a certain food. This reaction causes delayed hypersensitivity symptoms They are sometimes called “non-IgE food allergies”.
Examples include:- Eosinophilic [EE-oh-sin-oh-FILL-ick] esophagitis (EoE): a chronic (long-term) allergic or immune condition that causes swelling in your esophagus (part of the throat).
- Food protein-induced enterocolitis syndrome (FPIES) [eff-PIES]: an immune reaction in the gastrointestinal (GI) tract, that commonly causes vomiting, diarrhea, and lethargy. Symptoms usually appear about 1 to 4 hours after eating a food trigger.
- Allergic proctocolitis [prahk-toe-koh-LIE-tis]: an allergy to cow’s milk or soy proteins in formula or human milk that affects infants and is typically outgrown by age 1. Food allergies do not include intolerances (like lactose intolerance) or other types of immune-related responses to food (like celiac disease or Crohn’s).
- Immunoglobulin-E-mediated (IgE-mediated): With this type of food allergy, the body’s immune system makes antibodies called immunoglobulin E (IgE). IgE antibodies react with a certain food and cause immediate symptoms.
What Are the Symptoms of Food Allergies?
- Allergic reactions can range from mild to severe and involve the skin, mouth, throat, eyes, lungs, heart, gut, and brain.1
- Skin: hives, itchiness, swelling, flushing
- Mouth: swollen lips or tongue, itchiness, tingling or itchy feeling in the mouth
- Throat: swelling, tightness, difficulty swallowing
- Eyes: swelling around the eyes, itchiness
- Lungs (airways): difficulty breathing, wheezing, coughing
- Heart: passing out, dizziness, low blood pressure, shock
- Gut: vomiting, cramping, diarrhea
- Brain: passing out (linked with blood/heart system), change in mental status, severe sense of doom
- Severe symptoms affecting multiple parts of the body are called anaphylaxis [anna-fih-LACK-sis]. This reaction worsens quickly, and may lead to a medical emergency.
- Anaphylaxis must be recognized and treated right away with epinephrine to provide the best chance for improvement and to prevent serious, potentially life-threatening complications.
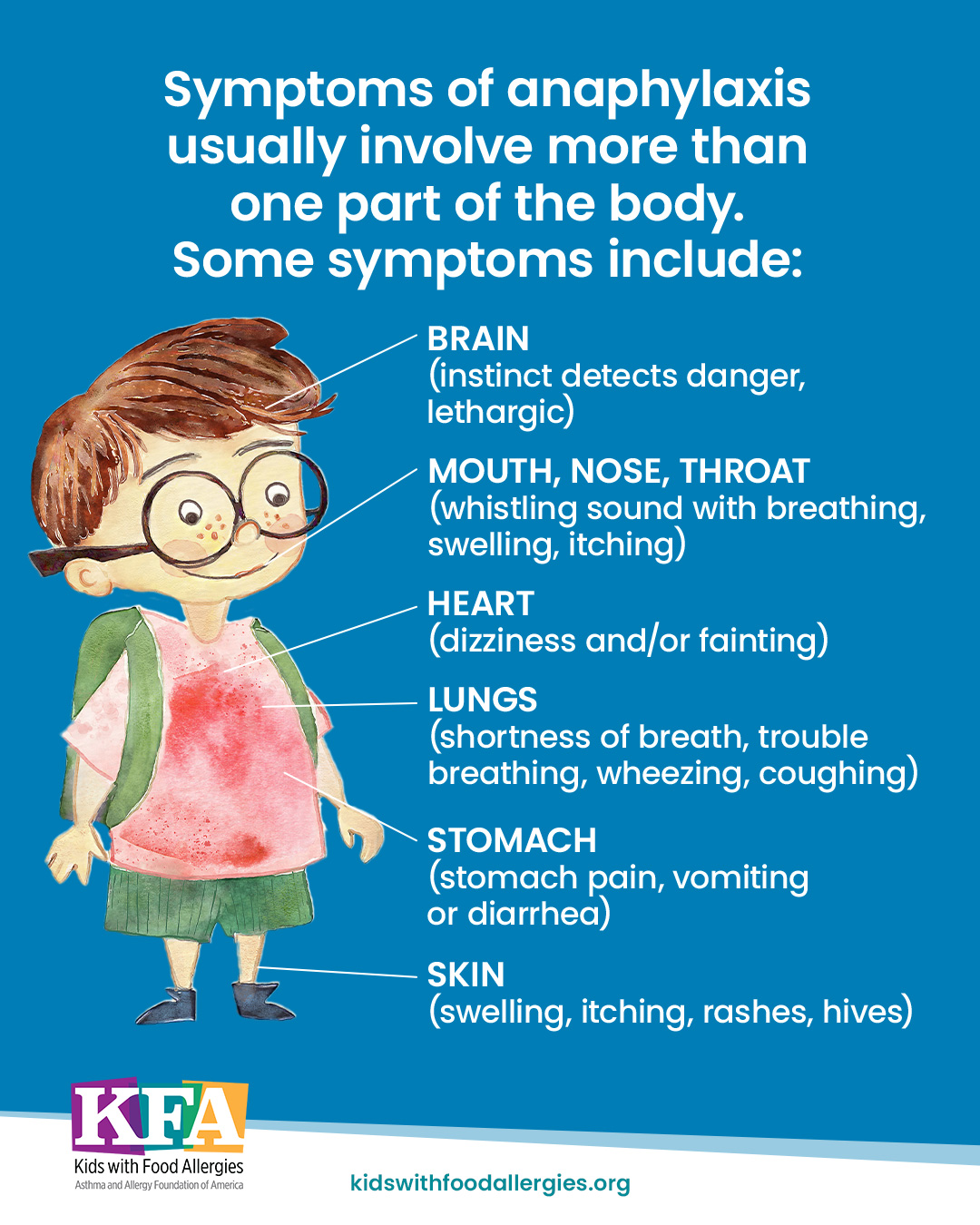
Symptoms of anaphylaxis
Anaphylaxis, a severe allergic reaction, can resolve quickly if treated right away with epinephrine.
How Common Are Food Allergies?
- As of 2024, nearly 22 million people have food allergies in the U.S. This equals about 6 out of 100 people.2,3
- About 18 million (7 out of 100) U.S. adults have food allergies.2
- About 4 million (5 out of 100) U.S. children have food allergies.3

22 million people with food allergies
Food allergy affects 18 million adults and 4 million children.

1 out of 17 kids has food allergies
This means 1-2 kids in every classroom may have food allergies.
- In 2024, 10 out of 100 non-Hispanic Black adults had food allergies, compared to 6 out of 100 non-Hispanic White adults.2
- 8 out of 100 non-Hispanic Black children have food allergies, compared to 5 out of 100 non-Hispanic White children.4
- Male children are more likely than female children to have food allergy, but female adults are more likely than male adults to have food allergy.2,3
- 6 out of 100 male children have food allergy, compared to 5 out of 100 female children.3
- 8 out of 100 female adults have food allergy, compared to 5 out of 100 male adults.2
- Around 1 in 700 people in the United States have EoE5
- EoE is more common in males than females, and most common in people aged 40-44 years old.5
- FPIES affects about 900,000 people in the United States, including about 1 in every 200 children and 1 in every 500 adults.6
Number of people with eosinophilic esophagitis (EoE)
Eosinophilic esophagitis (EoE) is a chronic (long-term) allergic or immune condition that causes swelling in your esophagus.
Number of people with FPIES
Food protein-induced enterocolitis syndrome (FPIES) is an immune reaction in the gut (gastrointestinal system) to one or more specific foods. The common symptoms are profuse vomiting and diarrhea.
What Are the Most Frequent Food Allergens?
- Nine foods cause most food allergy reactions in the United States:7,8,9
- Milk allergy affects 2 in 100 children and adults
- Egg allergy affects 1 in 100 children and adults
- Peanut allergy affects 2 in 100 children and adults
- Tree nut (for example almond, walnut, pecan, cashew, pistachio) allergy affects 1 in 100 children and adults
- Fish (for example bass, flounder, cod) allergy affects 1 in 100 children and adults
- Shellfish (for example crab, shrimp, scallop, clam) allergy affects 1 in 100 children and 3 in 100 adults
- Wheat allergy affects 1 in 200 children and 1 in 100 adults
- Soy affects 1 in 200 children and adults
- Sesame allergy affects 1 in 500 children and adults
Top food allergens
There is no cure for food allergies. To prevent allergic reactions, the food allergen needs to be removed from the diet.
- Milk is the most common food allergy in children, followed by egg and peanut.10
- Shellfish is the most common food allergy in adults, followed by peanut and treenut.10
- Milk, wheat, and egg are the most common food triggers of EoE.11
- Milk, oat, rice, and avocado are the most common food triggers of FPIES.12

Most common food allergens in children
The most common food allergens in children are foods that are typically in the American diet. Feeding babies these foods early helps prevent food allergy.

Most common food allergens in adults
You can develop a food allergy at any age. Many adults develop food allergies even without a prior history of allergies.
How Are Food Allergies Managed and Treated?
- Although treatments are available, there is currently no cure for food allergies.7
- Early recognition and learning how to manage food allergies, including which foods to avoid, are important measures to prevent serious health problems.7
- People with food allergies should carefully read food ingredient labels and always ask about ingredients before eating food prepared by other people.7
- Epinephrine is the first line of treatment for anaphylaxis.13
- It is critical to recognize and treat anaphylaxis early and without delay.
- People with diagnosed IgE-mediated food allergies should always have epinephrine with them. If anaphylaxis is suspected, epinephrine should be given right away and without delay to prevent severe complications (health problems).14,15
- If a person is having anaphylaxis, they should:
- Follow their Anaphylaxis Action Plan, a written plan created with a health care provider
- Use their epinephrine right away and without delay
- Get emergency medical care as needed if symptoms have not resolved14,15
Epinephrine to treat anaphylaxis
Epinephrine is safe to use. Give it right away for a severe allergic reaction.
ER visits due to anaphylaxis
You can prepare for anaphylaxis by having anaphylaxis action plan, keeping epinephrine with you at all times, and avoiding your allergens.
Do People Die from Anaphylaxis or Food Allergy?
- Food allergies are manageable and deaths are largely preventable.
- Deaths from anaphylaxis are extremely rare. Across the general population, anaphylaxis is the cause of about 1 out of every 2 million deaths each year.17 Most of these are caused by drug allergy.
- Deaths caused by food allergy reactions are even rarer. Fewer than 1 in every 10 million deaths are caused by food-induced anaphylaxis each year.17
Are Food Allergies Outgrown?
- Milk, egg, wheat, and soy allergies are often outgrown. Most people do not outgrow peanut, tree nut, fish, and shellfish allergies.10
Some food allergies are outgrown, while others persist
Some kids outgrow their allergies while others do not. There are treatments that help people tolerate their food allergen.

No cure for food allergies
You can live a healthy life with food allergies by avoiding your allergens, talking with your doctor about current treatments, and being prepared and confident to treat allergic reactions.
Download PDF

Food Allergy Fact
Feeding common food allergens to babies starting between 4-6 months of age lowers their risk of developing food allergy.
References
References
- Dribin, T. E., Motosue, M. S., & Campbell, R. L. (2022). Overview of Allergy and Anaphylaxis. Emergency Medicine Clinics of North America, 40(1), 1–17. https://doi.org/10.1016/j.emc.2021.08.007
- Bottoms-McClain, L., Giri, A., & Ng, A. (2026). Diagnosed Allergic Conditions Among Adults: United States, 2024. Centers for Disease Control and Prevention, National Center for Health Statistics. https://doi.org/10.15620/cdc/174634
- Ng, A., Giri, A., & Bottoms-McClain, L. (2026). Diagnosed Allergic Conditions Among Children Ages 0−17 Years: United States, 2024. Centers for Disease Control and Prevention, National Center for Health Statistics. https://doi.org/10.15620/cdc/174635
- Zablotsky, B., Black, L.I., & Akinbami, L.J. (2023). NCHS Data Brief, no 459: Diagnosed allergic conditions in children aged 0-17 years: United States, 2021. National Center for Health Statistics. https://dx.doi.org/10.15620/cdc:123250
- Thel, H. L., Anderson, C., Xue, A. Z., Jensen, E. T., & Dellon, E. S. (2024). Prevalence and costs of eosinophilic esophagitis in the United States. Clinical Gastroenterology and Hepatology, 23(2), 272-280. https://doi.org/10.1016/j.cgh.2024.09.031
- Nowak-Wegrzyn, A., Warren, C. M., Brown-Whitehorn, T., Cianferoni, A., Schultz-Matney, F., & Gupta, R. S. (2019). Food protein-induced enterocolitis syndrome in the US population-based study. The Journal of allergy and clinical immunology, 144(4), 1128–1130. https://doi.org/10.1016/j.jaci.2019.06.032
- S. Food & Drug Administration. (2025). Food Allergies. U.S. Department of Health and Human Services. https://www.fda.gov/food/nutrition-food-labeling-and-critical-foods/food-allergies
- Gupta, R. S., Warren, C. M., Smith, B. M., Blumenstock, J. A., Jiang, J., Davis, M. M., & Nadeau, K. C. (2018). The Public Health Impact of Parent-Reported Childhood Food Allergies in the United States. Pediatrics, 142(6). https://doi.org/10.1542/peds.2018-1235
- Gupta, R. S., Warren, C. M., Smith, B. M., Jiang, J., Blumenstock, J. A., Davis, M. M., Schleimer, R. P., & Nadeau, K. C. (2019). Prevalence and severity of food allergies among US adults. JAMA Network Open, 2(1), 1–14. https://doi.org/10.1001/jamanetworkopen.2018.5630
- Lee, E. C. K., Trogen, B., Brady, K., Ford, L. S., & Wang, J. (2024). The Natural History and Risk Factors for the Development of Food Allergies in Children and Adults. Current allergy and asthma reports, 24(3), 121–131. https://doi.org/10.1007/s11882-024-01131-3
- Godat, A., & Greuter, T. (2025). Food-related reactions in eosinophilic esophagitis: pathophysiology and treatment. Best Practice & Research Clinical Gastroenterology, 79, 102073. https://doi.org/10.1016/j.bpg.2025.102073
- Shah, S., Grohman, R., & Nowak-Wegrzyn, A. (2023). Food protein-induced enterocolitis syndrome (FPIES): Beyond the guidelines. Journal of Food Allergy, 5(2), 55–64. https://doi.org/10.2500/jfa.2023.5.230014
- David B.K. Golden, Wang, J., Waserman, S., Akin, C., Campbell, R. L., Ellis, A. K., Greenhawt, M., Lang, D. M., Ledford, D. K., Lieberman, J., Oppenheimer, J., Shaker, M., Wallace, D., Abrams, E. M., Bernstein, J. A., Chu, D. K., Horner, C. C., Rank, M. A., Stukus, D. R., & Burrows, A. G. (2023). Anaphylaxis: A 2023 practice parameter update. Annals of Allergy Asthma & Immunology. 132(2), 124-176. https://doi.org/10.1016/j.anai.2023.09.015
- Cardona, V., Ansotegui, I. J., Ebisawa, M., El-Gamal, Y., Fernandez Rivas, M., Fineman, S., Geller, M., Gonzalez-Estrada, A., Greenberger, P. A., Sanchez Borges, M., Senna, G., Sheikh, A., Tanno, L. K., Thong, B. Y., Turner, P. J., & Worm, M. (2020). World Allergy Organization Anaphylaxis Guidance 2020. World Allergy Organization Journal, 13(10), 100472. https://doi.org/10.1016/j.waojou.2020.100472
- Whyte, A. F., Soar, J., Dodd, A., Hughes, A., Sargant, N., & Turner, P. J. (2022). Emergency treatment of anaphylaxis: concise clinical guidance. Clinical Medicine, 22(4), 332–339. https://doi.org/10.7861/clinmed.2022-0073
- Michelson, K. A., Dribin, T. E., Vyles, D., & Neuman, M. I. (2020). Trends in emergency care for anaphylaxis. The Journal of Allergy and Clinical Immunology: In Practice, 8(2), 767-768.e2. https://doi.org/10.1016/j.jaip.2019.07.018
- Perez-Codesido, S., Rosado-Ingelmo, A., Privitera-Torres, M., Pérez Fernández, E., Nieto-Nieto, A., Gonzalez-Moreno, A., Grifol-Clar, E., Alberti-Masgrau, N., & Tejedor-Alonso, M. (2022). Incidence of Fatal Anaphylaxis: A Systematic Review of Observational Studies. Journal of Investigational Allergology & Clinical Immunology, 32(4). https://doi.org/10.18176/jiaci.0693
- Warren, C., Whittington, M. D., Bilaver, L., Kratochvil, D., Liu, R., Seetasith, A., Ko, S., Garmo, V., Kowal, S., Gupta, S., & Gupta, R. (2025). Estimating the societal economic burden of food allergy in the United States. Journal of Medical Economics, 28(1), 1–17. https://doi.org/10.1080/13696998.2025.2563462
Updated April 2026
Medical Review: April 2025 by John M. James, MD




